
When Pain Doesn't Fit in a Box: Understanding Persistent Pain
Why do painkillers sometimes stop helping?
Content:
A health psychologist's guide to why persistent pain sticks around, and what actually helps.
Most health conditions come with a certain amount of social shorthand. Say you're anxious, and people generally understand you're not making it up. Say you're feeling low, and there's a decent chance someone asks if you're okay and means it.
Pain doesn't usually get that same courtesy.
If your pain has gone on for a while, you've probably had to defend it at some point. Convince a doctor, someone from work, an old friend, sometimes even yourself, that your pain is real. Say "I'm not making this up" or "I'm not drug-seeking, I just need this to stop." Conversations about persistent pain tend to circle around proving the pain exists, rather than understanding why it's still here.
That's exhausting, and it isn't a reflection of your character.
There's a reason your pain hasn't gone away, and it isn't because you're weak, dramatic, or imagining things. It has to do with how your nervous system works, and once you understand it, a lot of what's been happening will start to make more sense.
This page walks through why persistent pain sticks around long after tissue has healed, and what tends to help. None of it promises a pain-free life. What it offers instead is a way to understand your pain well enough to live more fully alongside it.
"My scans look normal... so why am I still in pain?"
Health professionals draw a distinction between acute pain and persistent pain (sometimes called chronic pain). Acute pain shows up close to an injury and settles as the tissue heals; it's protective, and it does its job well. Persistent pain lasts well beyond normal healing time, often continuing long after the original tissue has healed as much as it's going to.
A clear scan doesn't mean nothing is wrong, and it doesn't mean you're imagining things. It usually means the story has shifted. Early on, pain was mostly about tissue damage. Later, the bigger factor is often how your nervous system is processing and producing pain signals, regardless of what's happening at the injury site itself.
Here's a way to think about it: has your body's alarm system become overprotective? Pain is generated by the brain as a protective response to perceived threat, not a direct readout of tissue damage. In persistent pain, that alarm system can become oversensitive, firing even when nothing is currently being damaged, a bit like a car alarm going off in strong wind rather than a break-in.
That doesn't make the pain any less real. It means the messaging system, not the tissue, has become the main problem.
"My pain doesn't take much to flare up": your nervous system's volume control
When you first hurt yourself, it's normal to feel soreness beyond the exact injury site. Stub your toe, and the ache can spread across your foot or up your calf, well past anywhere actually damaged. In effect, the volume around that area gets turned up temporarily. That's helpful: it encourages you to slow down while healing happens, and it usually settles as you return to normal activity.
Persistent pain often involves that same volume knob getting stuck. The nervous system becomes more sensitive over time, so smaller and smaller triggers, a new activity, a stressful week, even a change in weather, can set off pain that feels out of proportion to what's actually going on in your body. This is sometimes called sensitisation, and it explains why pain can flare from things that shouldn't logically cause much trouble at all.
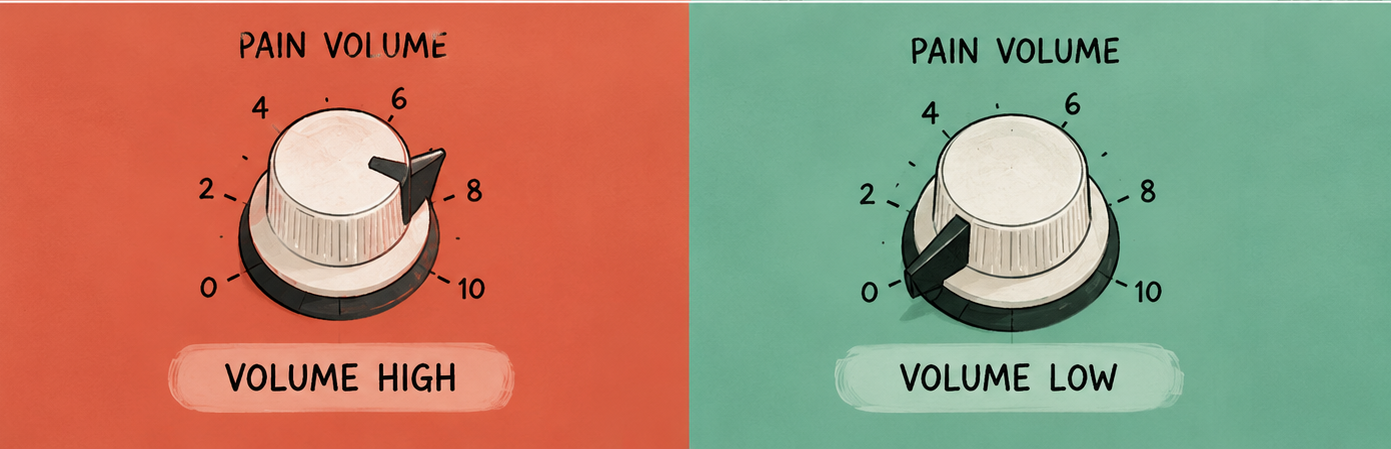
It also explains why emotions and pain are so closely linked. The chemicals your body releases during stress, poor sleep, or low mood run through very similar pathways to the ones involved in pain signalling, so a rough emotional stretch can turn the volume up further. The reverse is true too. Moments of enjoyment, connection, and genuine rest can help turn it back down. Neither direction means the pain is "all in your head." It means your nervous system is one interconnected system, not a set of separate switches.
Do you have good days and bad days? The boom-bust cycle
A familiar pattern for a lot of people with persistent pain: a good day arrives, and you try to cram in everything the bad days made impossible. Then the crash hits, sometimes hours later, sometimes the next morning, and you're stuck resting for days to recover. Once you feel a bit better, the cycle starts again.
There's a biological reason this keeps happening. Pushing the body to its limit floods it with stress chemicals as part of the fight-or-flight response, which in turn increases sensitivity to both pain and fatigue. Each round of the cycle can leave the nervous system a little more reactive than before, which is why boom-bust often feels like things are getting worse over time, even though what's really happening is a body getting more deconditioned and more easily triggered.
It also chips away at confidence. After enough crashes, it's natural to become wary of doing much at all, which brings its own problems. None of this means you should permanently do less. It means the rhythm needs to change, not the goal.
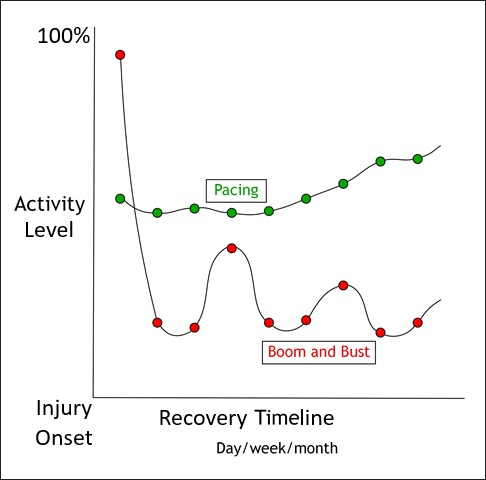
Why doing less today can help you do more next month: Pacing
Pacing is the antidote to boom-bust. Instead of doing as much as possible whenever you feel capable, you find a steady, sustainable activity level and build up from there, gradually, on a schedule rather than by how good today happens to feel.
In practice, that usually means starting smaller than you think you need to, staying consistent even on the good days, and increasing the load slowly, week by week, rather than day by day. A physiotherapist, exercise physiologist, or psychologist experienced in persistent pain can help you find that starting point and build a realistic plan from there.
Here's the part most pain resources leave out: you will not do this perfectly. There will be weeks you do too much because your child needed an early pickup, or too little because you slept four broken hours. That isn't a sign pacing has failed, it's what real life looks like. The goal was never a flawless routine. It's getting back to your plan without a pile of guilt attached to the detour.
When you can't call in sick: pacing for parents and carers
Most pacing advice assumes you can simply do less: reduce your hours, cancel a shift, hand a task to someone else. If you're caring for a child or another family member, that option often doesn't exist. There's no version of parenting where you tell a toddler you're operating at seventy per cent today. A newborn doesn't pause for a bad back. An ageing parent still needs help getting to the bathroom whether or not you slept last night.
This is one of the reasons pain in caregivers so often goes under-addressed: the standard advice doesn't fit the job. A few things tend to help instead.
Shift the goal from "less" to "different."
Rather than cutting back on what you do, change how you do it. Alternate which arm carries the nappy bag or the toddler. Sit on the floor for play instead of hunching over a cot. Break up long stretches in one position, feeding, rocking, folding washing, with small resets instead of pushing through until the task is finished.
Build more capacity than an average day requires.
A desk job has fairly predictable physical demands. Caregiving doesn't. A quiet afternoon can turn into carrying a full meltdown up two flights of stairs, or catching a parent who's lost their footing. Building strength and tolerance beyond what a typical day needs gives you a buffer for the days that aren't typical.
Your pain is real, and it isn't a reliable measure of ongoing harm.
Many carers push through pain because stopping isn't really on the table, then feel guilty when rest becomes unavoidable. Both things can be true at once: the pain is genuine, and a flare-up doesn't necessarily mean further damage is occurring.
Get to know your own patterns.
Was today's flare from a big lifting day, a rough night, skipped meals, or stress that had nothing to do with your body at all? Carers who track this tend to feel less blindsided by flares and more in control of them.
Protect whatever sleep you can get.
Generic sleep hygiene advice, a fixed bedtime, a dark room, no screens, often doesn't apply when you're up every few hours with a baby or doing overnight care for someone else. A more useful question is what's protecting the sleep you can get, and what's needlessly costing you more of it.
Your identity isn't the problem here, it's the reason this matters.
Many carers see themselves as the reliable one, the one who copes, the one everyone else leans on. Admitting to pain can feel like letting that identity down. It's worth flipping that around: managing your pain well is what protects your ability to keep showing up for the people who need you, not what threatens it
None of this is about doing less for the people in your care. It's about pacing the way you do it, so you can keep doing it for years, not just this week.
If you're nodding along right now, you don't have to work the rest of this out alone.
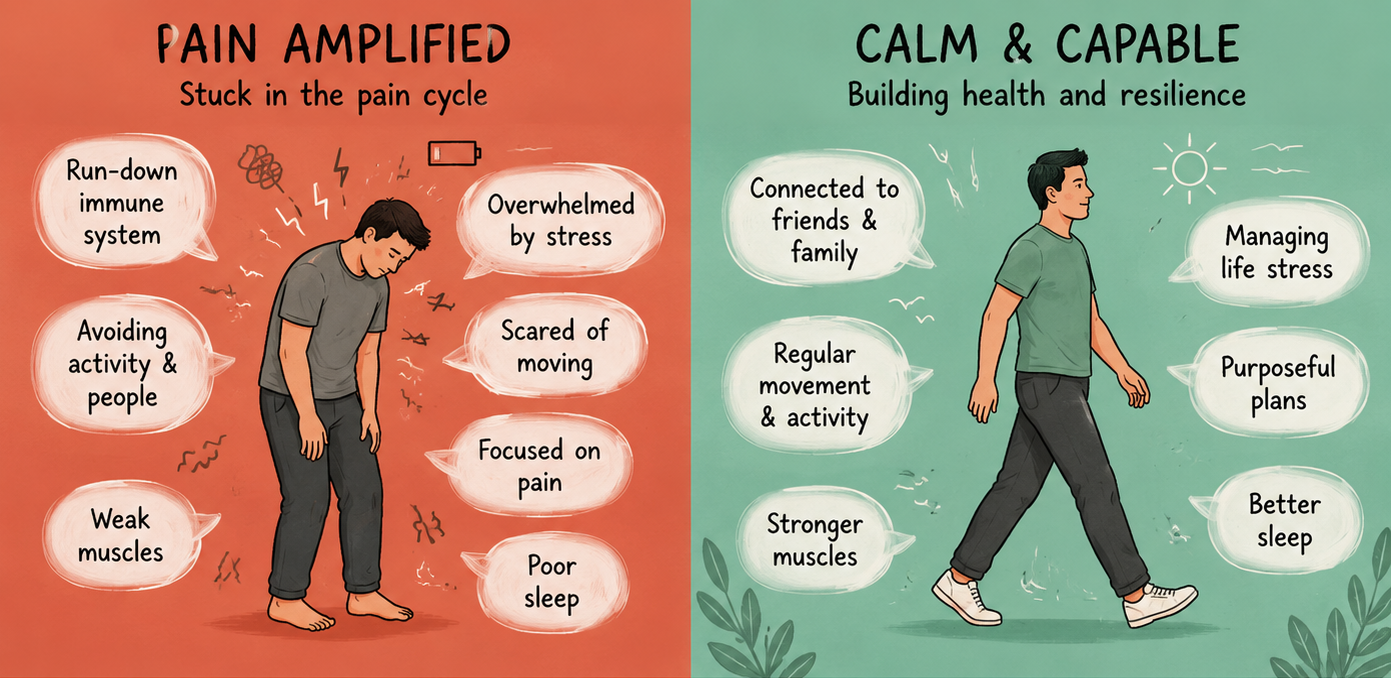
Why we stop moving, and why that backfires
Once pain shows up, it's natural to avoid whatever movement seems connected to it, hoping to protect the area. Over time, avoided movement leads to stiffness, weaker muscles, and a nervous system that's had less and less evidence that moving is actually safe, so it stays cautious. Meanwhile, the original injury may have long since healed.
A common version of this: someone hurts their back and is told bending is risky. Months later, the back has healed, but they still move stiffly, avoiding bending in ways that have nothing to do with any current injury and everything to do with a brain still treating bending as dangerous. Retraining that belief, gently and gradually, is usually what brings movement back, not more rest.
If you've been putting off rehab exercises because you're scared of making things worse, that fear makes complete sense. The real question underneath it is usually this: is this helpful pain, or unhelpful pain?
Is this helpful pain, or unhelpful pain?
Helpful pain is a normal signal that tissue is adapting to new load, similar to the soreness after using a muscle in an unfamiliar way. It typically eases within a day or two and doesn't sharply worsen each time you try the movement again.
Unhelpful pain points to genuine tissue damage: sudden, sharp pain that's significantly worse than before, especially alongside swelling, new weakness, or symptoms that don't settle with rest.
This distinction matters, and you shouldn't have to work it out alone. It's exactly what a physiotherapist or exercise physiologist is trained to help you figure out, particularly once pain has been around for a while and old injuries have long since healed.
You don't have to work this out alone
A physiotherapist or exercise physiologist plays a central role in persistent pain care, and for good reason. Working with one typically means:
Establishing a safe starting point for movement, without risking further damage
Building healthy movement habits and posture over time
Teaching your brain, through controlled and graded movement, that it's safe to move again
Reducing tightness through appropriate stretching
Strengthening the muscles that support the affected area
Identifying and correcting the compensating movement patterns that build up around avoided pain
That last point explains something a lot of people find confusing: pain that started in one spot and has since spread somewhere else. A knee that's ached for a year, and now the hip on the same side is sore too. A lower back injury that's somehow become a shoulder problem.
Picture a tree with one weak branch. The rest of the tree doesn't leave that branch to fend for itself: other branches grow to take on extra weight, roots shift to compensate, and the whole structure adjusts around the part that isn't pulling its weight. Over time, the parts doing the compensating start to strain too. The original branch might even be fine by now, but the tree has reorganised itself around it regardless.
Bodies do something similar. A physio or exercise physiologist can help work out which "branch" started the problem and which ones are just compensating, then build a plan around the whole structure rather than only where it currently hurts.
As a health psychologist, my role isn't to prescribe exercises or replace that work, it's to work alongside it: helping with the fear, the frustration, the motivation gaps, and the mental side of learning to trust your body again while your physio or exercise physiologist handles the physical rebuilding.
Why do painkillers sometimes stop helping?
Many people start with medication as their main strategy, and understandably so. It's accessible, it's fast, and early on it can genuinely help. Over time, though, some people notice the same dose doesn't do what it used to, or that medication takes the edge off without changing how much pain interferes with daily life.
There are a few reasons for this. It's worth understanding them, though any decisions about your medication should always sit with your GP or prescribing doctor, never changed on your own.
• The body can build tolerance to some pain medications, so the same dose has a smaller effect over time.
• Medication targets pain signals; it doesn't address a sensitised nervous system, deconditioned muscles, or a boom-bust pattern, all of which keep the volume turned up regardless of what's in your system.
• Research on persistent pain consistently points to medication working best as one part of a broader plan, alongside movement, pacing, and psychological support, rather than as a stand-alone fix.
None of this is a suggestion to stop or reduce anything you've been prescribed. It simply explains why medication alone tends to plateau, and why combining it with the other pieces on this page usually makes more difference than increasing a dose.
Movement, confidence, and behaviour change
Everything above points to the same underlying shift: from protecting yourself against pain, to slowly showing your nervous system that movement is safe again.
That happens through small, repeated evidence, not big leaps. Each time you move a little without a flare spiralling out of control, your nervous system logs it as safe. Do that consistently, and the volume gradually starts to come down. Confidence isn't something you talk yourself into, it's something you build through small wins that stack up over weeks and months.
This is often the hardest part, not because people don't understand what to do, but because knowing the plan and consistently living it are two very different things. That gap, between the plan on paper and the plan in your actual week, is where a lot of the psychological work happens: the motivation dips, the setbacks, the old fears that resurface right when things start improving.
What recovery actually looks like
It's worth being upfront about something: recovery from persistent pain rarely means becoming pain-free. For some people, pain reduces significantly. For others, it settles into the background of a life that's otherwise full again. Neither outcome is guaranteed, and anyone promising you a pain-free result is promising something pain science can't back up.
What tends to be realistic is a different relationship with your pain. One where a flare doesn't derail your whole week. Where you know your own patterns well enough that flares feel less frightening than they used to. Where pain has a gradually smaller say in what you do with your day.
That's not a quick fix. It's closer to a long game: consistent, unglamorous, built slowly. But it's a game a lot of people learn to play well.
Ready to make sense of your pain?
If any of this sounds like your experience, that's a good sign, not a bad one. It means there's a well-understood process behind what you're going through, and well-understood processes can be worked with.
I'm Gordon Wong, an AHPRA-endorsed Health Psychologist and the psychologist behind Socra Hub, a telehealth practice supporting adults across Australia. My approach draws on Acceptance and Commitment Therapy, and I work alongside your GP, physiotherapist, or exercise physiologist rather than replacing them; you keep your existing care team, and we add the piece that's often missing.
